January is a good time to start helping
your clients plan for their annual giving. With the year-end flurry of
donations still fresh in many clients’ minds, you may discover that clients
will welcome your suggestion to make 2023 the year to get organized early,
particularly as economic headwinds make planning especially important.
A conversation that benefits everyone
Among the many benefits of discussing
charitable giving with your clients is that your clients will see you as an expert,
especially when you have a close working relationship with the team at the Community
Foundation. Your philanthropic clients want to learn how they can make a
difference through their charitable activities, and they are expecting their
advisors to be ready to help them structure and plan their giving. Indeed, for
years, research has shown that a proactive advisor who offers options for
incorporating philanthropy into financial and estate plans inspires client
loyalty, even across client generations.
The Community Foundation advantage
Advisors frequently comment that
they’re surprised to discover the many ways the Community Foundation can help
their clients, especially compared with national donor-advised fund programs
affiliated with brokerage houses or financial services firms.
Often the greatest needs are right here at home, and working
with the Community Foundation is the very best option for ensuring that your
clients are informed and impactful philanthropists.
The Community Foundation is unparalleled in its ability to
be flexible and responsive, providing outstanding, personal service designed
around your clients’ needs while always respecting your role as your client’s
primary advisor.
Options for every client’s unique situation
Here are just a few of the ways we can
work with you as you plan for 2023:
Wills and trusts
A client can establish a bequest to a
fund at the Community Foundation through a will or trust or through a
beneficiary designation on a qualified retirement plan or life insurance
policy. The Community Foundation will provide proper
bequest language.
Retirement plan beneficiary
designations
Bequests of qualified retirement plans
can be extremely tax efficient. Funds flowing directly to a client’s fund at
the Community Foundation from a retirement plan after the client’s death will
not be subject to income tax or estate tax.
Family philanthropy
Consider encouraging clients to involve
their children and grandchildren in philanthropy, especially when the clients
are working with the community foundation through a family donor-advised fund
or other collaborative vehicle. We offer a variety of personalized
giving services to make the charitable giving
experience rewarding and impactful.
Income tax planning
Remind clients that they are eligible
for an income tax deduction for lifetime charitable gifts, and the gifted assets are no longer subject to future estate
taxes.
Complex giving
Consider more complex giving vehicles,
including charitable remainder trusts, and charitable gift annuities. The Community
Foundation can work with you to establish these structures to help facilitate
your clients’ charitable giving goals and meet the clients’ financial and tax
goals at the same time.
We look forward to working with you in
2023!
Congress passed the much-anticipated,
$1.65 trillion-dollar omnibus spending bill known as the Consolidated Appropriations Act of 2023 (“CAA”) December 23, 2022. At more than 4,000 pages, the Act includes a
wide range of provisions that impact multiple sectors.
Of particular interest to attorneys,
accountants, and wealth managers who advise philanthropists are the provisions starting midway through the bill. The
bipartisan legislation often referred to as “SECURE 2.0” is included in the CAA
legislation. As background, SECURE 2.0’s provisions build on the original
SECURE Act of 2019 (“SECURE” stands for “Setting Every Community Up for
Retirement Enhancement). SECURE 2.0 includes the Qualified Charitable
Distribution (QCD) enhancements that have been in the works for many months.
Here are three key provisions affecting
philanthropists in the new law:
–Taxpayers may now make a one-time
$50,000 QCD transfer to a charitable remainder trust (CRT) or other
split-interest gift such as a charitable gift annuity (CGA). These are the “Legacy IRA” provisions. Note that the law
effectively mandates that the CGA or CRT be created solely for the purpose of
receiving a QCD because the new statute requires that the vehicle contain only
IRA assets.
–The required minimum distribution
(RMD) age (previously 72) increased to 73 on January 1, 2023. The age will
increase to 75 beginning on January 1, 2033. While this provision is not
directly tied to charitable giving, it will nonetheless impact your clients’
overall financial plans and potentially affect the timing and strategy of their
philanthropy. As a reminder, “required minimum distribution” (RMD) refers to
the mandated amount that a taxpayer must withdraw from qualified retirement
plans, which include IRAs as well as 401(k)s and other tax-deferred retirement
accounts.
–The annual per-taxpayer $100,000 QCD
cap is now slated to be indexed for inflation, which will allow taxpayers to
give even more from their IRAs directly to charity.
Here’s what has not changed:
–Eligibility for making a QCD still
starts at 70 ½. This allows taxpayers who are not yet required to take IRA
distributions under the RMD rules to still take advantage of the QCD technique
without the income tax hit on the distributed funds while also removing those
funds from liability for future estate taxes.
–Taxpayers required to take RMDs can
still count QCDs toward their RMDs, thereby avoiding the usual income tax hit
on RMD dollars.
–Charities eligible to receive QCDs
include designated funds, field-of-interest funds, and scholarship funds at the
community foundation, but still not donor-advised funds.
In fewer than five minutes with Jane Hunt you can feel her passion. Her positive energy and nature are palpable and before long, you’re wrapped up in one of the many causes she supports to help her community.
Hunt is the daughter of Johnelle and J.B. Hunt, founders of J.B. Hunt Transport Services, Inc., one of the largest transportation and logistics companies in the world.
“I saw my dad taking care of people, from his employees to a stranger on the street,” said Hunt. “He lived out his faith and always cared for the poor. He was my example, and I try to live my life like him. I knew from a very young age that I was going to help people too.”
One of Jane’s deepest passions is supporting early childhood education. “I have worked with several different nonprofit programs, and we all recognize we must address immediate needs while also working on the root of the problem. Experience demonstrates that early intervention pays off in the long run,” she said.
Hunt is a teacher by trade. “I loved teaching junior high,” she said. “It was apparent that the strongest students were not inherently smarter than their peers, they simply had the advantage of having been in a quality childcare or pre-K setting. There is so much data that supports the ripple effect of quality early childhood education. Healthy babies, toddlers and preschoolers become strong, capable adults.
“And it isn’t just little ones that need support. There must be a holistic approach. You have to create an environment around the babies and toddlers with good teachers, good childcare centers and good family support.”
One of the charitable funds Hunt initiated at Arkansas Community Foundation is the Early Childhood Champions Fund. The fund supports quality early childhood programs for children up to five years of age as well as scholarships for preschool teachers. The fund also extends the pre-K and Headstart day past 5 p.m. so that parents can work. Anyone who values early childhood education can donate to the fund.
Because of her influence, energy and commitment, hundreds of working families and their children have benefited from full-day, quality, early childhood education.
“I truly believe that supporting early childhood education is the ‘magic bullet’ to solve social issues and make our community a better place,” said Hunt. “Investing in our children is an investment for all of us.”
A group of committed citizens in Horatio, Arkansas, decided to start improving early childhood development for their community. Through research and community data, they raised funds to create innovative solutions to address gaps in early development for the town’s children. Now, they are making a huge difference for children’s development and family health in this southwest Arkansas town with a population of 984.
Children who don’t meet developmental expectations and are not ready for kindergarten are considered at-risk. Understanding where a community’s most vulnerable children live, along with knowing specific areas for improvement, allows schools, neighborhoods and cities to work together and make informed decisions.
In March 2019, community members in Sevier County participated in a first round of Early Development Instrument (EDI) assessments*. These assessments are a tool meant to identify areas for improvement for vulnerable children.
In Horatio, the EDI assessments revealed gaps in the areas of physical activity, gross and fine motor skills and overall social competence. To address these gaps, a subcommittee of community members began raising funds to improve local recreational spaces, and partnered with companies to elevate childhood development as part of business culture and customer experience.
Beth Tody is the regional coordinator for Excel by Eight in the area. She worked alongside schools, families and communities to help them understand the results of the EDI assessments and determine solutions for addressing the gaps. “Parks and recreational spaces have amazing benefits for children’s physical development as well as their emotional development,” said Tody. “That notion is what drove our project design.”
One of the first areas of improvement was the local parks. “Through our conversations with community members, we heard that there simply weren’t enough safe, free places for families with young children to play, aside from joining competitive sports teams,” said Tody. “We know that childhood obesity turns into adult obesity, which exacerbates other chronic health conditions. We know that if children aren’t physically ready for school by kindergarten, then they struggle to learn.”
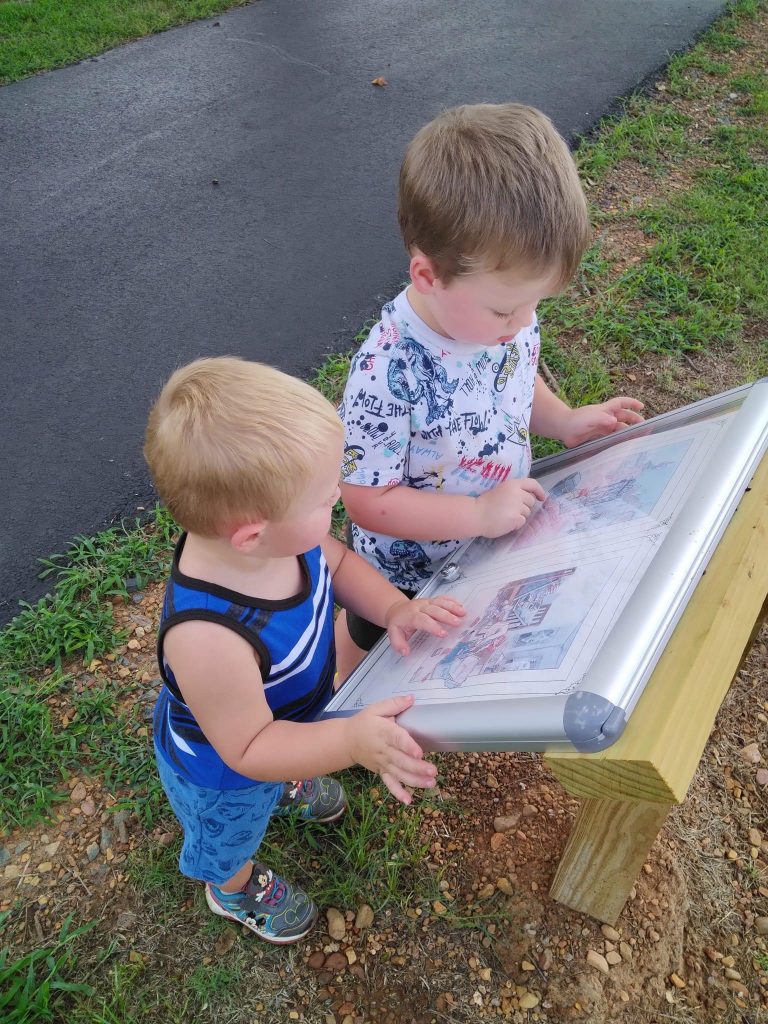
One innovative solution to address both the lack of access to free places to play and to help children be ready for kindergarten was the installation of a StoryWalk® in partnership with Save the Children.
“Imagine walking down a trail with a child, and you come upon a page from a children’s book. As you continue walking, you find another page, and then another, and you begin to realize you’re following a story,” said Tody. “This has been so fun and educational for our town.”
The subcommittee also set up “busy boards” to help toddlers with their fine motor and problem-solving skills. These simple boards also help children practice real-life skills to ready them for their first year of school, like figuring out how to use zippers and buckles.
The story walks and busy boards were the first to be installed at two parks and a library. Then bilingual signage and book distribution locations were added around town. “We wanted our efforts to be family centered and easily accessible for all families, regardless of home language or ability to pay,” said Tody.
“Once the story walks and busy boards were finished, we saw local businesses step up to help and create their own fun ways to support our efforts,” she said. “We ended up adding book trees at Main Street Kitchen and Simple Simon’s Pizza, and Prime Country Meat market provided after-school snacks and meals. Now, in addition to a new soccer field being in the works, we are exploring putting in a farmers’ market and a new playground to attract families to Hendrix Park. This project has been a great example of how both public and private investment in a community can lead to positive change.”
Research shows that access to recreation not only helps promote physical health for children and families, but also social-emotional health. When children are able to regulate their emotions, they are able to focus and follow directions in school-based settings. According to Tody, “Providing these spaces where children can play together helps them foster early friendships with other children. It also gives them the confidence they need in their development to be successful in their relationships with friends, family and at school.
“This entire initiative took a small group of dedicated people committed to making a difference for our children. And if it can be done in Horatio, Arkansas, it can be done anywhere.”
*EDI assessments measure children’s physical health and wellbeing; social competence; emotional maturity; language and cognitive skills; and communication skills and general knowledge. The results are combined so a community has a snapshot of how children are developing across neighborhoods, including areas of early development that need more support and in which parts of the community resources should be targeted.
When Heidi Klappenbach visits new moms through Family Connects of Union County, she pulls from the memory of when her own children – now grown – were babies.
“I really think that what I love about the program is just being able to encourage moms,” said Klappenbach, who is a Family Connects of Union County visiting nurse.
Family Connects of Union County is a pilot program by the Medical Center of South Arkansas and Arkansas Children’s Hospital based on the Family Connects International model, based in Durham, N.C. Its mission is to support new mothers in Union County, connecting them and their growing families with the community resources they need to start out safe and healthy.
All new moms in Union County are eligible and can schedule home visits after giving birth. Visits are typically scheduled when babies are about three weeks old, often coinciding with the time new dads are returning to work and when family who comes to help with the new baby may be going home. The visit from a Family Connects nurse is meant to offer support as the new mom settles into motherhood, giving her and her baby resources for the best, safest start possible. There are physical assessments of both mother and baby, and the visiting nurses can help, if needed, with feeding issues.
Klappenbach brings a portable scale so she and the mother can check the baby’s weight and talk about general growth and development.
There is a self-assessment for postpartum depression, which affects 50 percent of all new mothers, according to Stone. “Many of them don’t realize the depth of postpartum depression until they do our questionnaire, and we talk about it, and they’re like, ‘Oh my gosh, I really am having problems,’” said Alison Stone, a registered nurse who supervises the program. In those cases, mothers may be referred back to their obstetrician or to a local counseling agency for relief.
“We tell them we can reach out and set them up and just kind of get them over this hump,” Stone said.
Some mothers have confided to visiting nurses that they borrowed car seats to take their babies home from the hospital or that they co-sleep because they don’t have a bassinet. The nurses can explain safe sleeping practices and can provide some of the necessary baby equipment to families in need.
They can also ask about fire, smoke and carbon monoxide alarms in the home.
“A lot of places don’t have those so we try to connect them to the resources they need to get them,” said Stone. “It’s kind of everything in their environment. We’re assessing everything and trying to help, to meet whatever needs they have.”
Klappenbach started her nursing career in labor and delivery and postpartum care before taking time off to raise her own children. She returned to nursing about nine years ago and started working with Family Connects when it started in 2019.
“She’s very motherly,” said Stone, “I think that’s a huge positive for us because she’s very loving, very easygoing, and they feel comfortable, I think, with her coming into their home because she does have a very nurturing personality.” Klappenbach enjoys the opportunity to combine her nursing and parenting skills to help new mothers through Family Connects.
She remembers the “purple crying” stage, often labeled colic, when 2-3 week old babies resist soothing. She can reassure moms that this stage usually ends by about 2 months, and she can tell them about comforting babies with the five S’s – swaddling, sucking, swinging, shushing and laying baby across your lap on his stomach. “Then that goes into talking about Shaken Baby Syndrome, as far as it being OK to lay the baby in the crib and go get a drink of water when you need to take a little break,” Klappenbach said.
She can dispel myths about things they may have heard from their grandparents, like that they can spoil their babies by holding them.
Stone noted that Klappenbach has occasionally picked up on health issues and referred babies for follow-up care. “There was one baby that we sent to Children’s, and it did need some medical interventions. That was a good catch on the mom and Heidi’s part because it was not caught in the hospital. Heidi has had a lot of good catches.”
The nurses are there to give a quick but comprehensive look at each newborn’s unique environment.
“This home-visiting program is supposed to be like a little light touch,” Stone said. “We can’t fix everything, but we can address concerns and fix the biggest issues.”
Klappenbach visits as many moms as she can before they leave the hospital, so that when she visits them at home she’s a familiar face. She knows some women are reluctant to have a home visit out because they worry the nurses will critique their parenting.
“But I just love telling them they’re doing a good job,” said Klappenbach.
When it comes to improving the lives of children, it’s natural to look for ways to meet their immediate needs — from basic material needs such as food and clothing to books, toys, and other items that are both fun and beneficial to their learning and development.
What’s more challenging to tackle are the systemic reasons why some children do not have access to these resources and what can be done to ensure all children have a strong start to life, even before they are born.
Excel by Eight [E8] is an initiative that partners with families and communities to improve health and education outcomes for Arkansas children prenatal to age eight. Established in 2011 as the Arkansas Campaign for Grade-Level Reading, its mission was to ensure all children read at grade level by the end of third grade. With the support of more than 30 partner organizations, Arkansas Campaign for Grade-Level Reading received national recognition for its work to help improve parent and community engagement, school readiness, classroom instruction, attendance and summer learning.
Despite these successes, there was more progress to be made.
Executive director Angela Duran began her role with the Arkansas Campaign for Grade-Level Reading in 2011. She oversaw its transition to Excel by Eight in 2019.
“We realized that we needed to broaden our efforts to ensure all children meet their full educational and health potential,” she said.
The Resource Grid To visualize its broader focus, Excel by Eight has developed a resource grid to identify all the areas that must be addressed so that children have what they need to thrive.
“We liken it to a power grid,” Duran explained. “Some parts may be incomplete or malfunctioning, or the connections may be frayed or broken altogether. An unreliable or patchy flow of resources can result in a range of developmental delays, with long-lasting consequences for children’s health and well-being.
“What we want to do is make sure families and communities are equally plugged in and have full grids with all of the connections working.”
The resource grid is arranged into four categories — family, community, education and health — and includes home visiting; parenting resources; safe and affordable housing; physical, mental, and oral health; early care and education; and much more.
Across Arkansas, there are already programs and practices designed to help children, starting from birth, achieve their full educational and health potential. Duran said that unfortunately, the grid of resources families need is often unevenly distributed, making it difficult for them to access these critical family, community, education, and health supports.
“Our role at Excel by Eight is to transform our state’s systems so families and communities can overcome barriers that prevent children from achieving their full potential,” she said.
Three-Legged Stool Excel by Eight consists of a team of policy makers, healthcare professionals, educators, nonprofit leaders, and community developers committed to increasing children’s health and education outcomes in three primary ways. This “three-legged stool” encompasses partnering with and investing in local communities, impacting public policy at the state level, and building public support around the importance of the earliest years of a child’s life.
Communities Excel by Eight communities are local models for change. E8 currently works in six Arkansas communities: Conway County, Independence County, Jefferson County, Little Rock, Sevier County and Union County.
“Building and supporting local models for change allows E8 to highlight community successes and identify policy barriers that can be addressed at the state level,” said Duran. “While every E8 community is at a different stage in their planning and implementation, each local steering committee has assessed available resources and gathered input from residents as part of the process.”
In October, Excel by Eight brought its communities together in Batesville for its semiannual learning community. This convening allows communities to learn from each other and share best practices.
As host community, the Independence County steering committee led a site visit to a local school district to demonstrate LENA Grow, a 10-week program intended to measure and improve adult-child interactions in early care. Public preschool centers at all four school districts in Independence County have adopted the program.
“LENA Grow is just one example of how Data Walks — which is our community input process — informed this decision to focus on oral language and literacy skills,” Duran said. “Our role is to help parents, educators, health professionals, and other community members in all of our communities identify gaps in their resource grids and develop strategies for improving child outcomes.”
Policy The Excel by Eight Foundations Collaborative (E8F) is the policy leg of the three-legged stool. E8F has developed a policy agenda that builds on existing knowledge of how to best support families with young children. Duran said they chose the name “Foundations” for their policy work because prenatal to age three is critical for brain development and sets the foundation for a child’s health and education outcomes.
“We are investing in our youngest children because we know that’s when the brain develops fastest,” Duran said. “We are looking comprehensively at both health and education outcomes for children, starting with prenatal care.”
A child’s experiences in the first three years are the bricks and mortar of brain development, with more than one million new neural connections forming in an infant’s brain every second. According to the Center on the Developing Child at Harvard University, responsive relationships and positive experiences build sturdy brain architecture that becomes the foundation for core social emotional intelligence, early executive functioning and self-regulation, and literacy.
While these critical skills and experiences begin at home, Duran said they can also be provided through effective programs and policies.
“It’s not only infants, toddlers, and families who benefit when we start early — it’s entire communities. When we invest in the first three years of a child’s life, we build a strong foundation for their future learning, behavior, and health and reduce the need for more expensive interventions later.”
E8 Foundations’ policy agenda can be categorized into three areas: Healthy Beginnings, Supported Families, and High Quality Child Care and Early Learning. This policy agenda builds on existing research and knowledge of how to best support families with infants and toddlers.
“We want children to have healthy beginnings, and we want families to feel supported and have access to high-quality child care and early learning experiences,” Duran said.
Public Support Because Excel by Eight does not provide direct services to children, generating public support around its goals is not always as straightforward as it can be for organizations that work directly with children. Systemic change doesn’t happen overnight, but Duran is optimistic about the progress that has been made so far.
“We want to continuously make the connection between the community and the policy work so that people understand our vision to make Arkansas a state where all children have a strong start to reach their full potential.
“We know that it’s going to take a while to achieve our goals,” Duran said. “But we know we can do it. And we are in it together.”
Garrett Dolan of Tyson Foods
Op-ed by Garrett Dolan, Ph.D. Senior Manager, Corporate Social Responsibility Tyson Foods
The provision of child care influences who is available to work, when a person is able to work, where they can work, and especially, why they work.
In Arkansas and across the nation, there are very few affordable care options available. The annual cost of tuition exceeds $10,000 per child. Not to mention, it costs over $4 million to build a new licensed facility. These costs far exceed what a working family can afford and are the primary reasons why there is limited availability.
Running parallel to the child care shortage is an “intense and growing shortage” in labor participation. Tyson Foods experiences this problem with fewer candidates being able to work, higher rates of turnover and increases in absenteeism. Child care is one of the top reasons why these trends are deepening.
Collectively, we have a real opportunity to improve our state’s future if we aggressively address child care together. With smart investments, we can expand the labor pool, reduce reliance on government welfare, and increase school readiness for children. It requires transformational thinking with the supply of governmental incentives especially related to the cost barriers of building new facilities and paying tuition. Parents need tuition subsidies that are realistic and sufficient enough for them to choose to go back to work.
At Tyson Foods, we are working hard to figure out our company’s role in addressing child care and doing more to serve the communities where our team members live and work. We strive to be the most sought-after place to work and ensure team members have the tools and resources they need to be successful. We have piloted two on-site child care programs in Texas and Tennessee to help us learn more. Meanwhile, it is Arkansas where we call home and employ more than 20,000 team members.
Let’s join together and move with purpose to bring about the systemic changes needed.
For many rural communities, the school district serves as the economic, cultural, and social hub of the town. Pea Ridge School District — also referred to as Pea Ridge School Community — has adopted a community-focused model that meets the needs of all Pea Ridge residents, not just the students.
Alex Jackson, special projects coordinator for Pea Ridge School District, oversees community initiatives such as The Blackhawk Pantry. The pantry is open every Thursday morning to students, families, faculty, and community members to pick out kid-friendly meals, fresh produce, protein, and other resources at no cost.
The Northwest Arkansas town can be considered a “bedroom community,” as most of its residents travel south to Bentonville and other nearby cities to work. The school district is Pea Ridge’s largest employer and enrolls 2,496 students in pre-K through 12th grade.
Assistant superintendent Anne Martfeld has a 25-year career in education and began working in the Pea Ridge School District four years ago. At the time, the district was beginning construction on its new high school building. The new construction — combined with a grant from the Walton Family Foundation — served as a blank slate for the district, allowing Pea Ridge School District to explore how they could use the new facility to meet the needs of the community while integrating an innovative learning opportunity for students. Community Clinic Pea Ridge became the foundation of the district’s community-centered model.
“We partnered with Community Clinic to have a school-based health center in the high school which would be adjacent to the medical care professions classroom,” Martfeld said. “Our grant from the Walton Family Foundation helped us think about the connection of community and school and how we as a district could serve our community in a holistic way.”
Community Clinic Pea Ridge offers primary and acute care, basic lab tests, wellness checks, immunizations, sports physicals, return-to-play care, and other services to the community of Pea Ridge and the surrounding area.
In addition to being open to the entire community, Community Clinic Pea Ridge offers a shuttle for students. This transportation option allows children to get sports physicals, wellness exams, and other routine health care services without their parents or caregivers having to miss several hours of work to get them to and from appointments in Bentonville.
The clinic served as a launch pad for Pea Ridge School District to build additional inclusive spaces that provide students with real-world experiences while meeting a community need. Alex Jackson is the special projects coordinator for the district and oversees the clinic and other community initiatives, including The Blackhawk Pantry.
Community Clinic Pea Ridge is adjacent to the medical care professions classroom, giving students the opportunity to gain real-world experiences while meeting a community need.
Every Thursday morning, The Blackhawk Pantry is open to students, families, faculty, and community members to pick out kid-friendly meals, fresh produce, protein, and other resources at no cost. To date, the Northwest Arkansas Food Bank has donated more than 25,000 pounds of food to the initiative.
“Our district social worker, Amanda Shackelford, wanted to have a closet where students could access food,” Jackson said. “I am known for going big, so we cleared out our old records room and essentially created a free grocery store.”
Since opening in February 2022, The Blackhawk Pantry has served an average of 100 people per week, totaling more than 3,800 visits. Jackson wants to ensure the pantry is available to anyone who needs it and simplifies the process of meeting families’ needs by minimizing asks of patrons. Students in the district make up 40% of visits.
The Blackhawk Pantry also serves as a resource center in partnership with the Northwest Arkansas Food Bank and Community Clinic where experts on social services program are on-site and available to answer any questions.
“To me, having a community-centered school involves all of those pieces working together to make it successful,” Jackson said. “And that comes from having strong relationships with our students, our teachers, and our external and internal stakeholders.
“When people from the community step foot on our campus, we want them to be able to envision themselves as being a part of our community school.”
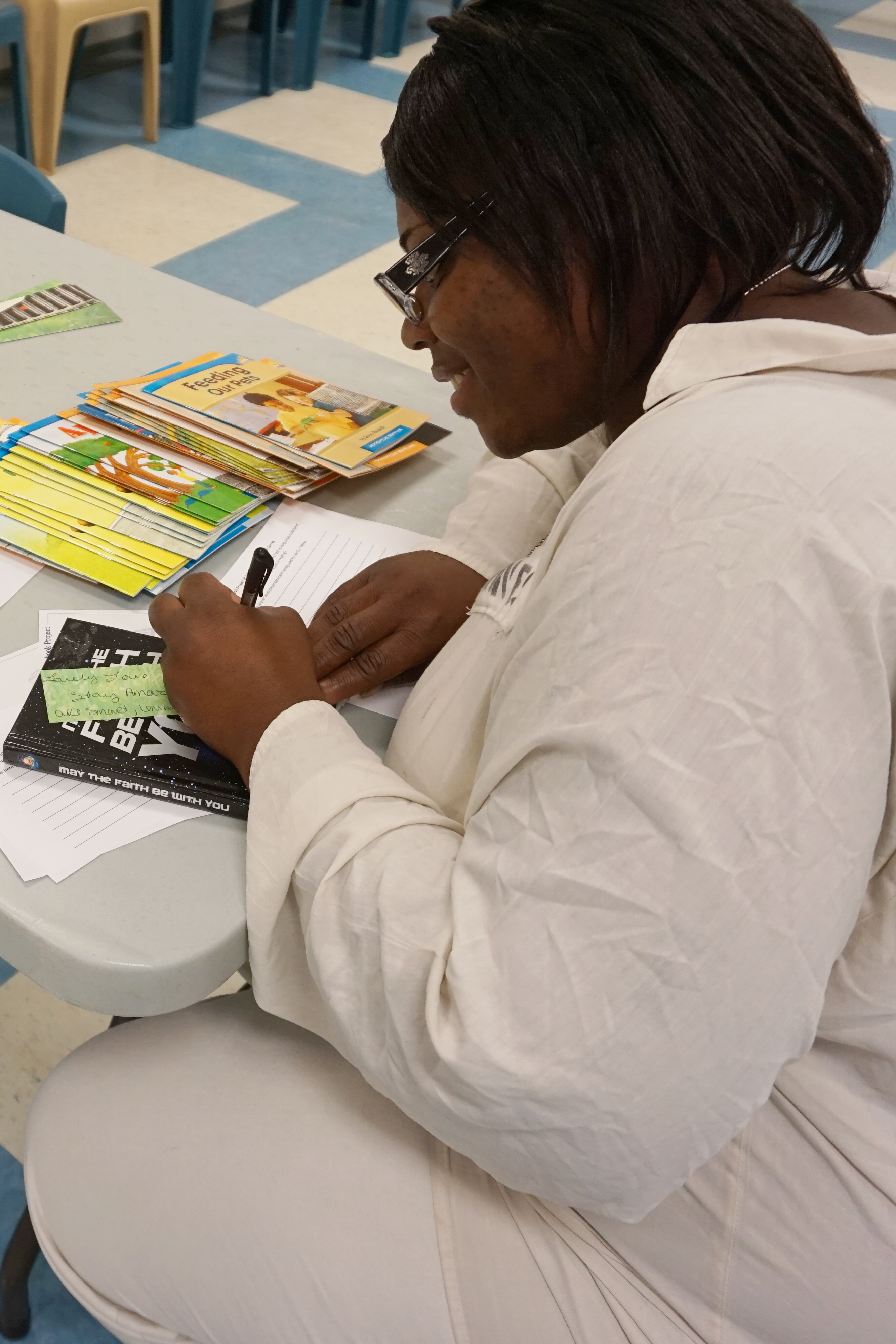
Undrea “Gem” Jones is a former inmate and volunteer. She goes into prisons regularly to record parents reading books they have chosen for their children. Jones understands the complexity of parents’ feelings as they read.
Undrea “Gem” Jones was released from prison after 21 and a half years on Feb. 26, 2019. She always knew she would go back in — but as a volunteer for the Storybook Project of Arkansas. She wants to be a part of helping parents and grandparents form and foster bonds with the children in their lives the way volunteers helped her.
“It was a momentous event for me because it was coming full circle,” she said. “That was a whole experience that I had been waiting to have for a very long time.”
Jones was sent to prison for a crime she committed at the age of 16. Her son was 2 years old. The Storybook Project of Arkansas, a nonprofit prison outreach that allows volunteers to record inmates reading to their children, was already underway at the Arkansas Department of Corrections-McPherson Unit when she arrived.
Experts, like those from the American Academy of Pediatrics, point out that reading to children not only boosts their language skills, it also strengthens their relationships with their parents.
Books have seen Jones through some of the hardest times in her life, including her own childhood.
“I love books. I excelled in academia,” she said. “There was a lot of trauma that I was dealing with at that time, and books were a safe-haven for me. I read anything that transported me from my present circumstances.”
She couldn’t physically pull her son onto her lap and snuggle him for reading time while she was in prison, but the Storybook Project of Arkansas allowed her to give him the gift of her voice.
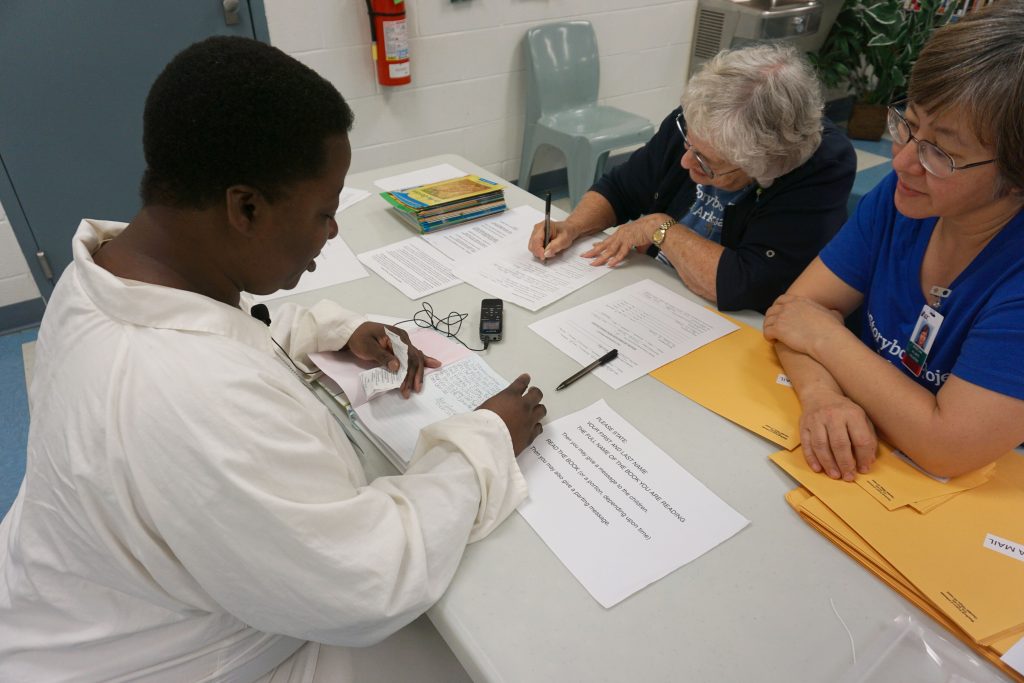
Jones and other volunteers from the outreach visit prisons four times a year, said Denise Chai, who leads the Arkansas program.
“We bring in a whole bunch of books, and they choose one,” said Chai. “They will write a message in the book, and then they go and sit down with a volunteer and they’re recorded, giving a message Then they read the book and give another message at the beginning. After we leave the prison, we burn that to a CD, because we’re not quite digital, and we mail the book and the CD to the child.”
Jones doesn’t remember any of the books she chose to read to her son.
“I don’t remember the books because you’re going through so much in the process at that moment,” she said. “It’s amazing, but it’s also really difficult because you want to say so much to your child, but at the same time you want to hold it together and send love and encouragement, and you’re holding a broken heart because you can’t be there. You would have to prepare yourself so you would not be overcome with just the gratitude and appreciation and broken-heartedness — and get through it.”
Choosing books to share with him, however, was simple. “I heard another volunteer say we had so many different, beautiful books, and she said, ‘How do they choose which book they want to read?’” said Jones. “I said, ‘The book chooses us.’ During the whole process as my child grew older, I found a book always picked me for what I was going to read to him.”
She remembers asking him to read a book about Puerto Rican evangelist Nicky Cruz when he was old enough, and to let her know what he thought of it. She didn’t read the book to him, but he did write a report to share his thoughts when he finished on his own.
“He had the foundation of reading from the storybooks that I sent him,” she said.
That book, like others they shared during her sentence, created common ground for them, helping foster a bond that can be lost when parents and children are separated for long periods.
Jones considers herself lucky because some of the people she met in prison didn’t have custody of or contact with their children; her son was in the care of family, and they made sure he heard about her and that she saw him when possible. The recordings he received of her reading to him linked them while they were apart, sometimes serving as conversation starters when they could be together.
She hasn’t discussed the Storybook Project with her son and won’t hazard a guess about what it might have meant to him. She is a proud mom, though.
“My son has a love of academia, and he went to college on an academic scholarship. He loves knowledge,” she said. “He is career-focused, and he’s in a committed relationship. He has never been touched by the criminal justice system. He is an awesome man.”
The Storybook Project, she said, helped her be a better mother.
“It wasn’t just about reading a book or sending a book or recording to our child,” she said. “To us, it’s everything. We get to send a piece of ourselves to our children, some of them we haven’t ever seen, some of them we haven’t seen in years or months,” she said. “That one moment that we got the opportunity to be a normal parent was —– is — just something that is priceless.”
Market declines and inflation have made 2022 a challenging year
for some clients to fulfill their traditional giving objectives.
With annual inflation hovering at 8% (and no relief in sight) and
liquidity less than ideal, cash may be hard for donors to part with. Giving
stock may also be hard to swallow, at least psychologically, in a down market.
For example, assume shares of a client’s stock have dropped 15% over the last
quarter, from $200 per share to $170. If the client has been intending to make
a $10,000 gift to charity this year, last quarter the client could have
accomplished that with a gift of 50 shares. Now, though, the client will need
to give nearly 59 shares to hit that $10,000 target. Realizing that it will
“take more shares to do the same good,” your clients may be less inclined
to give depreciated stock shares to their donor-advised funds and other
charitable recipients.
So, with money tight and stock perhaps painful to give, your clients may be considering alternatives to cash or securities for their gifts to charity. Be aware of the IRS rules to both meet the clients’ objectives and stay in Uncle Sam’s good graces.
A high-level understanding starts with the $5,000 threshold for
documentation that appears on IRS Form 8283,
titled Noncash Charitable Contributions. This form is required to be filed with
any tax return claiming such a deduction.
Substantiation of value up to $5,000 is routine and consistent
with securities (i.e., acquisition
and contribution dates, fair market value of the item(s) and method of value determination).
Requirements for gifts up to $500 are less stringent.
Real estate, closely-held stock, art, jewelry, or vehicles valued
at $5,000 or greater require more specifics. They’re also subject to greater
scrutiny if the donor is audited or questioned.
Consider the additional documentation requirements:
–From the donor (your client): the type of gift, description,
physical location and a third-party appraisal of value.
–From the appraiser: a signed declaration on the tax form
describing their qualifications and identification number; that they do this
work regularly; and where they can be located.
–From the recipient (the charity, sometimes known as the “donee”):
signed confirmation of qualification, receipt, federal identification number
and a commitment to document and notify if disposition occurs within three
years. (The Community Foundation is accustomed to filing this
documentation for donors’ gifts to funds.)
Your clients also need to know that meeting the requirements for
declaring value rests with them and not their tax preparer,
recipient organization or appraiser. In the recent case of Heinrich
C. Schweizer v. Commissioner, a donor/taxpayer was found
liable for reimbursements and penalties related to a decade-old donation of art
first valued at $600,000—later reduced by more than 50%—and exacerbated by the
IRS’s determination of participants’ roles and responsibilities. Tax advisors
continue to be reminded of the intricate requirements to substantiate
hard-to-value gifts such as conservation easements, watching carefully to see
how taxpayers can win
valuation arguments with the IRS.
So while a high-value donation of real property to your client’s
donor-advised at the community foundation or a little-used auto to benefit a
charity is admirable and relieves the pressure on
making traditional cash or securities gifts, patrons should take a vigilant and
“donor beware” approach to alternative gifting. While beauty is in the eye of
the beholder, value and deductibility are determined by others.